Osteoarthritis of the shoulder happens when the surfaces inside the shoulder joint become worn and the cartilage gradually disappears. This wearing away gets worse over time, causing abnormal friction, pain, swelling (fluid accumulation and bursitis) and stiffness (limited movement in the shoulder). The pain happens not only when you move the shoulder, but also and often more disturbingly, at night. The wearing away of the cartilage is irreversible, and there is no cure for osteoarthritis. The only thing you can do is slow it down.
Osteoarthritis is a degenerative condition, which means it is linked to wear and tear, but there are also extrinsic factors that can accelerate the progression of the disease. The main causes are:
- A history of recurrent shoulder dislocation
- A rotator cuff tear
- Surgery on the shoulder joint
- Fracture (of the humerus or glenoid rim (shoulder blade))
- A rheumatic disorder (e.g. chondrocalcinosis, rheumatoid arthritis)
The first step in treating osteoarthritis is to give medical treatment i.e. pain relief. This is often combined with hygiene and dietary measure to alleviate the pain. Injections of hyaluronic acid are also required to lubricate the joint and protect the damaged cartilage. This is sometimes combined with physical therapy.
There are two types of shoulder osteoarthritis :
Concentric (primary) :

This is the standard form of osteoarthritis where the cartilage has worn away from the head of the humerus and glenoid rim. The rotator cuff tendons are intact and still working. It usually affects patients in their sixties. X-rays reveal a humeral head nicely centred within the joint, and an MRI confirms no damage to the rotator cuff tendons.
Eccentric (secondary) :

This is a particular form of osteoarthritis where the rotator cuff tendons have been torn. The humeral head is no longer held in place by the tendons and moves off-centre. X-rays show the humeral head raised above the glenoid rim of the shoulder plate. An MRI confirms a rotator cuff tear.
Osteonecrosis of the humeral head :

Osteonecrosis of the humeral head is a complication of a bone infarction, which can have wide-ranging causes (steroid therapy, haemoglobin disorders, Lupus or other auto-immune diseases) or even no known cause. It causes pain and stiffness. The condition can be diagnosed with standard x-rays for advanced cases, or with an MRI for early cases.
Treatment is always surgery.
Surgery is indicated when medical treatment no longer has any effect.
It involves a total shoulder replacement.
The diagnosis is based on the clinical history, with patients often clearly describing pain for many years and a gradual loss of range of motion in the joint. The night pain becomes more and more disabling. There is often an identifiable cause (e.g. dislocation, shoulder surgery, rotator cuff tear).
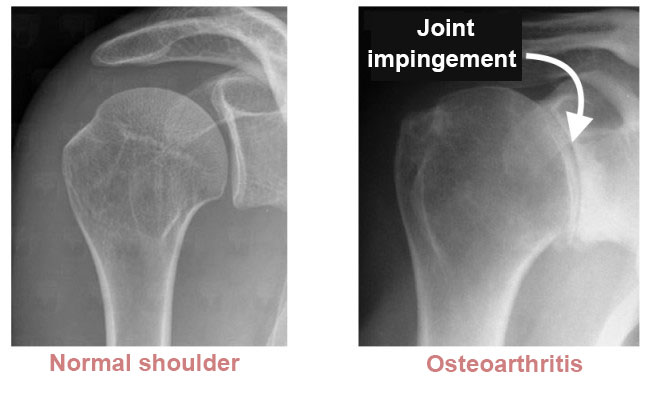
An x-ray is essential for confirming the diagnosis. The images are taken from the front with the joint in three rotations (lateral, medial and neutral) and from the side. They reveal joint impingement i.e. a narrowing of the distance between the joint surfaces indicating loss of the cartilage.
Multi-slice imaging (MRI or joint scan) will also be used to determine the extent of damage to the rotator cuff and plan any surgery.
These results will be used to classify the osteoarthritis as concentric or eccentric.
A Total Shoulder Replacement is indicated when medical treatment no longer has any effect. The procedure offers functional treatment with the sole aim of improving the patient’s quality of life. It is therefore ultimately up to the patient to decide whether to go ahead with the operation. Dr Lévy will try to explain what will happen in either scenario, with and without the surgery. Surgery should be recommended for patients whose daily lives are disabled by the shoulder pain, especially if the night pain is preventing the patient from sleeping. This disability should be significant, and not just occasional. There is no hard and fast rule, because every patient is different. There is no age limit for a total shoulder replacement, but it should be avoided in young patients because the only limitation of the procedure is the life span of the implants which will eventually have to be replaced if the patient is too young; although sometimes, there is obviously no other option. Fortunately, there have been great improvements in implant quality and they now have a much longer life span.
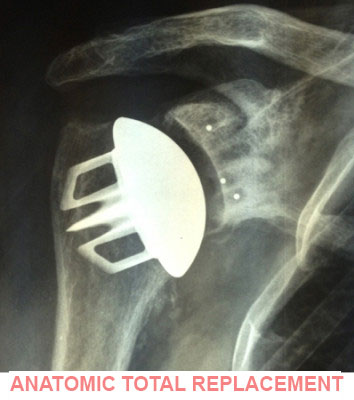
For concentric osteoarthritis, Dr Lévy will use a technique known as an anatomic total shoulder replacement. The implant works the same as a normal shoulder but needs the rotator cuff tendons to be intact. The tendons are what will allow the shoulder to move after the surgery. If the rotator cuff tendons are torn, the implant will not work.
For eccentric osteoarthritis, he will use a reverse total shoulder replacement. This is a special type of implant that changes the centre of rotation of the joint, allowing the shoulder to work without the need for the rotator cuff tendons. The deltoid muscle does all the work, allowing the shoulder to still move. Unfortunately, this type of implant has a shorter life span than anatomic implants.

Ultimately, the need for surgery will be decided after a long discussion between the patient and surgeon.

You should keep your arm in a sling night and day for 4 weeks after the surgery. If you are very careful or when taking a shower, you can remove your arm from the sling and hold it against your body. Rehabilitation will start as soon as possible, with the aim of keeping the joint mobile. It will start with pendulum exercises several times each day. The only movement you are not allowed to do during the first month is lateral rotation (turning the arm outwards). Nurses will come to change your dressing for 2–3 weeks. You should do your exercises every day to help your shoulder recover as much mobility as possible. The skin staples will be removed between day 1 and 21.
POSTOPERATIVE CHECK-UPS :
30-DAY CHECK-UP :
By now you will have started physiotherapy to help restore the range of motion in the joint. The swelling should have begun to go down a little bit, and it will be less painful. The night pain should in principle have disappeared. Dr Lévy will examine the scar, your mobility, and determine whether there is any residual pain. He will look at your new x-rays, and make any necessary adjustments to your recovery plan for the next few months. You should be able to start driving again after 45 days.
4-MONTH CHECK-UP :
Your rehabilitation should now be aimed at restoring full range of motion, including rotation, and supporting the muscles. You should be getting used to your implant, but will still be aware it is there. Your muscles will not quite have regained full strength, and you can improve it with either exercises at home or physiotherapy. Dr Lévy will give you advice on how to avoid damaging the shoulder.
Depending on your recovery, he may allow you to resume running, cycling and swimming.
12-MONTH CHECK-UP :
In principle, by now you should no longer have any pain and be able to move your shoulder however you want, without thinking about it. However, each shoulder is different and Dr Lévy will give you specific advice on whether you can resume sports. It is possible to play many sports after a total shoulder replacement (e.g. tennis, golf, skiing, running). Your surgeon will give you a schedule for gradually resuming these activities. Contact sports (e.g. football, rugby, judo) should be avoided.
RESULTS :
Shoulder replacement surgery gives an excellent result in over 90% of cases, with patients experiencing no or very mild pain. Patients will often forget about their total shoulder replacement within 6–12 months.
The average life span for a total shoulder replacement is 15–20 years for anatomic implants, and 10 years for reverse implants. After this time it will need to be replaced. The second operation is often more complicated than the first time, and the results not quite as good.
You should see your surgeon for a check-up every year, with x-rays to check for any complications. This will just be a short appointment so he can check the scar, your movement, any pain and take some x-rays.
You must take every precaution against infections, and treat any infection as quickly as possible (dental, sinus, urinary infections etc.). This is because the bacteria could migrate to the shoulder at any time and infect the implant, in which case the only option will be to have it replaced.