
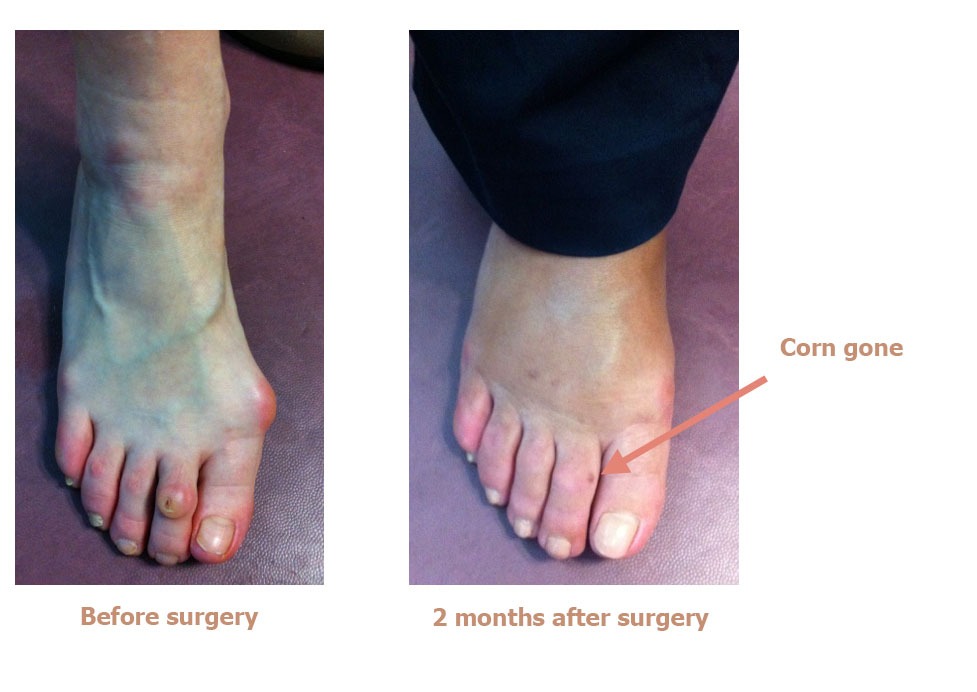
Hammer toe is a common foot problem. It refers to a deformity of one or more toes where they are bent and cannot be straightened, causing them to rub against the inside of shoes. The top of the hammer-shaped toe rubs against the top of the shoe, causing burning pain and corns on the top of the toe.
 The deformity can also place excessive pressure on the ball of the toe. It mainly affects women in their fifties. The problem is often related to hallux valgus (bunions), but can also occur with a hollow foot, rheumatoid arthritis or other foot problems. Without surgery to remove the deformity, treating the corns with pedicures is pointless. In fact, the corns will come back very quickly because the toe will still rub against the shoes.
The deformity can also place excessive pressure on the ball of the toe. It mainly affects women in their fifties. The problem is often related to hallux valgus (bunions), but can also occur with a hollow foot, rheumatoid arthritis or other foot problems. Without surgery to remove the deformity, treating the corns with pedicures is pointless. In fact, the corns will come back very quickly because the toe will still rub against the shoes.

In the early stages of the condition, the deformed toe is supple and painless. Then it becomes stiff and cannot be straightened. Eventually, if left untreated, it can lead to dislocation of the metatarsophalangeal joint and crippling pain in the sole of the foot.
The corn can get infected and lead to arthritis (infection) of the toe.
The surgery is usually carried out as an outpatient procedure (day hospital)
ANAESTHESIA :
The procedure will be performed under local anaesthesia. The anaesthetist will first give you a local anaesthetic into the toe so you won’t feel any pain or discomfort during the surgery. The surgeon will then top-up the anaesthesia once the area is numbed. This top-up is used to prolong the effects of the anaesthesia for 10–12 hours. You will therefore not be in any pain when you return home. When you are discharged from the clinic, you will be given a prescription for pain relief.

PERCUTANEOUS SURGERY :
Dr Lévy will perform the operation using micro-incisions for inserting instruments just 2mm in diameter. This means the scars will be barely visible to the naked eye. If there is still flexibility in the hammer toe, the surgeon will cut the extensor tendon and release the metatarsophalangeal joint (a procedure known as arthrolysis). If the toe can no longer be straightened, he will also remove some bone from the end of the distal phalanx (top of the toe). It is this excess length that is causing the deformity. By removing a few millimetres of bone, the surgeon is creating space for the toe to straighten out again. No fixation material is used (e.g. screws, staples).
Throughout the operation, Dr Lévy will take x-rays to check what is happening and make sure the osteotomy is as accurate as possible.
Once finished, he will apply a compression dressing that will act as a splint for 8–10 days, during which you should not remove or loosen the bandage or get it wet.
You will then spend a few minutes in the recovery room so your vital signs can be monitored, before returning to your room and waiting to be discharged.
Dr Lévy will prescribe any medication needed to alleviate any pain after the surgery. When you are discharged, you will be given a copy of your medical file explaining that you must bring back the dressings to your next check-up, along with any other instructions and the date and time of your next appointment when you will have another x-ray.
After being discharged, you will be able to walk with orthopaedic shoes that Dr Lévy will have prescribed for you during the preoperative consultation.
Dr Lévy will give you an appointment for a check-up in 8–10 days’ time. During this time, you must wear the orthopaedic shoes which are designed to relieve pressure on the forefoot.

POSTOPERATIVE CHECK-UPS :
8–10 DAY CHECK-UP :
Dr Lévy will remove the dressing and affix a splint to hold and keep the toe straight. This splint will make sure the bone heals in the correct position. You will must continue wearing the orthopaedic shoes for one month.
1-MONTH CHECK-UP :
The dressing and splint will be removed. You will return the orthopaedic shoes and can start wearing loose-fitting footwear (e.g. trainers, plimsolls). The swelling may take 2–3 months to go down. You will also be given some exercises to do at home to help recover the full range of motion in your toes.
3-MONTH CHECK-UP :
This appointment is to check how your toes are healing. However, each case is different and you may be given advice on how to improve your condition and speed up your recovery.
You may also be given further appointments, if the surgeon thinks it is necessary.
REHABILITATION :
The benefit of percutaneous surgery is less stiffness after the procedure. In most cases there is no need for rehabilitation therapy. At your first check-up appointment, Dr Lévy will give you some exercises to do at home. These exercises are designed to restore the range of motion in the joints, massage the scars to prevent any deep-seated adhesions, and get you walking again normally.
In some cases, he may want to prescribe you some sessions with a physiotherapist.







