There are four main ligaments that give stability to the knee.
The collateral ligaments, which sit just beneath the skin on either side of the knee (medial and lateral collateral ligaments) and provide frontal plane stability.
The cruciate ligaments which are inside the joint (anterior and posterior cruciate ligaments) and provide stability in the sagittal plane.
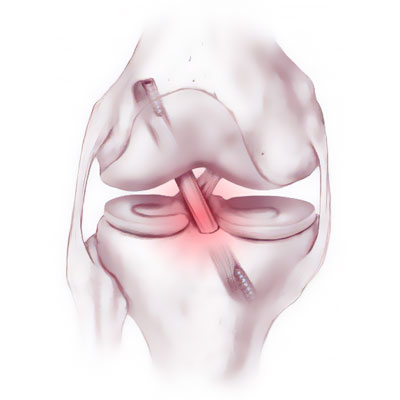
The anterior cruciate ligament links the anterior part of the tibia to the posterior part of the femur. It stops the tibia from sliding out in front of the femur and stabilises the knee during rotation.

The anterior cruciate ligament can tear during an accident (playing sport, at work or at home) and lead to a knee sprain. It often involves a high degree of trauma. The most common causes are skiing and football accidents. There are around 20,000 cases each year in France. The knee twists and the patient often both feels and hears a short but sharp snap.

At first the pain is very bad and the patient feels the knee give out. After a few seconds, the patient can stand but is unable to place any weight on the leg, which is too unstable.
In the minutes or hours after the trauma, the knee begins to swell badly due to bleeding inside the joint caused when the blood vessels ripped. This bleeding inside the joint is called haemarthrosis.

The injury may be accompanied by a meniscus tear or damage to one or both of the collateral ligaments.
PROGRESSION :
The ligament is unable to heal itself and restore the anatomy to normal. If left untreated, the knee will usually remain loose and continue to give way, which may get worse over time. With a loose knee, any pivoting movements during sport risk causing further episodes of instability, which feel like a new sprain, and the looseness may lead to progressive meniscus tear or damage to the cartilage (osteoarthritis).
SURGICAL CONSULTATION:
The aim of the preoperative consultation with the surgeon is to establish a diagnosis. Dr Lévy will examine the knee to determine how much the cruciate ligament is damaged. This will involve a full examination of the knee to check for any meniscus tear or other ligament laxity.
X-rays and an MRI will be used to help plan the surgery.

Depending on the damage and its cause, Dr Lévy will decide what is required. He will explain what will happen during and after the surgery, as well as any potential complications. This will include advice on the length of remission and when you can resume any sports.
ANAESTHETIC CONSULTATION:
Once the indications have been confirmed, one of Dr Lévy’s assistants will give you an appointment with the anaesthetist who will look after you during the surgery. The anaesthetist will examine you and prescribe any additional tests that may be needed before the surgery. He or she will also explain how the anaesthesia works and the best method for you. The procedure is usually performed under general anaesthesia, with a regional catheter in the thigh for reducing the pain immediately after the procedure.

SMOKING :
It is essential to stop smoking one month before and after the surgery. This is because a mass influx of nicotine reduces blood flow, slows down the healing process and makes it harder for the new cruciate ligament to fuse with the bone. You may use extended-release nicotine patches to help with the withdrawal symptoms.
The surgery will be performed as an outpatient procedure. Dr Lévy preforms most ligamentoplasties using the 4-strand semitendinosus technique (ST4) and a short graft. The graft is harvested using a short 2cm incision over the inside edge of the tibia.

The rest of the procedure is performed arthroscopically (guided using a camera). The surgeon makes tunnels in the tibia and femur using special instruments. These tunnels are positioned exactly at the insertion points of the torn cruciate ligament. The graft is carefully measured then the tunnels made exactly the same size. The graft is secured using two anchors fixed to the femur and tibia. These anchors support the graft until it has fused with the bone.

You will be able to get out of bed either the same evening or the next morning, depending on the time of your surgery. You will wear a soft knee brace for 15 days to provide initial support and assistance for your knee.

This video demonstrates the procedure:






