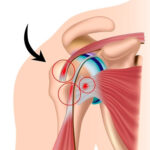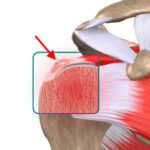
A torn rotator cuff is a very common problem. It happens when one or more of the four shoulder tendons (supraspinatus, infraspinatus, subscapularis or teres minor) gets torn.

It affects adults over 40 either as a result of a degenerative tendon condition and/or trauma (direct impact, sprain, dislocation). An early diagnosis is important to avoid residual pain. under general anaesthetic and is performed as an oupatient procedure.
There are two types of rotator cuff tear:
Traumatic (dislocated shoulder, a violent forced movement causing the shoulder to snap)
Degenerative (wear, ageing), although the two types are often interlinked.

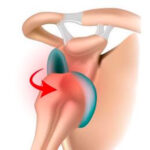
The symptoms of a torn tendon are pain, loss of active movement and loss of strength in the shoulder. It becomes harder to move the arm, and daily activities become painful or even impossible to do.
THE MAIN SIGN IS NIGHT PAIN THAT PREVENTS YOU FROM SLEEPING
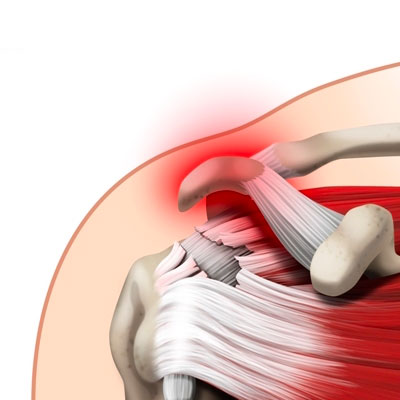
If you leave it too long without treatment, the tendons shrink (making the surgery more complicated) and the muscles irreversibly waste away, meaning you are less likely to recover fully. A tear can also spread to the other rotator cuff tendons. The aim of repairing the rotator cuff is to alleviate the pain and restore mobility and strength to the shoulder. It will also prevent progressive deterioration of the joint and its function.
SURGICAL CONSULTATION
The aim of the preoperative consultation with the surgeon is to establish a diagnosis. Dr Lévy will examine the shoulder to determine which tendon or tendons are affected. This involves a comprehensive examination to test the tendons one by one and identify which ones are affected by the tear.
He will look at X-rays and an MRI (or joint scan) to quantify the tear, muscle quality and retraction. This information will be used to plan the surgery. Depending on the damage and its cause, Dr Lévy will decide what is required.

He will explain what will happen during and after the surgery, as well as any potential complications. This will include advice on the length of remission and when you can resume any sports.
If the shoulder is stiff, you may be offered a few sessions of physiotherapy to loosen the joint and prepare the shoulder for the surgery.
ANAESTHETIC CONSULTATION:
Once the indications have been confirmed, one of Dr Lévy’s assistants will give you an appointment with the anaesthetist who will look after you during the surgery. The anaesthetist will examine you and prescribe any additional tests that may be needed before the surgery. He or she will also explain how the anaesthesia works. The procedure is always performed under general anaesthesia, together with locoregional anaesthesia to minimise any postoperative pain.
SMOKING :
It is essential to stop smoking one month before and after the surgery. This is because a mass influx of nicotine reduces blood flow, slows down the healing process and makes it harder for the tendons to fuse with the bones. You may use extended-release nicotine patches to help with the withdrawal symptoms.
 You should keep your arm in a sling day and night for one month after the surgery. If you are very careful or when taking a shower, you can remove your arm from the sling and hold it against your body. You should not raise the arm or actively move it away from the body. Depending on the complexity, Dr Lévy may give you some exercises involving strictly passive movement, starting 10 days after the operation. If the repair was tricky and the tendons particularly retracted, physiotherapy will start after the one-month check-up. In all cases, Dr Lévy will ask you to do some pendulum exercises to prevent the shoulder getting stiff.
You should keep your arm in a sling day and night for one month after the surgery. If you are very careful or when taking a shower, you can remove your arm from the sling and hold it against your body. You should not raise the arm or actively move it away from the body. Depending on the complexity, Dr Lévy may give you some exercises involving strictly passive movement, starting 10 days after the operation. If the repair was tricky and the tendons particularly retracted, physiotherapy will start after the one-month check-up. In all cases, Dr Lévy will ask you to do some pendulum exercises to prevent the shoulder getting stiff.
POSTOPERATIVE CHECK-UPS :
30-DAY CHECK-UP :
By the time you attend this first check-up, the majority of patients say that the spontaneous night-time pain has disappeared. You should still avoid sleeping on the shoulder but sleep on your back or on your other side. This appointment is the last time you will need to wear the sling. Dr Lévy will make sure the wounds are healing well and check your passive movement. An x-ray will be used to check that the implants used to secure your tendons have stayed in place. At this point the surgeon he whether you can begin active assisted physiotherapy, and increase your passive then active range of motion, depending on the pain. You must continue to massage the scars to prevent any subcutaneous adhesions from forming.
4-MONTH CHECK-UP :
At this appointment, Dr Lévy will check the range of motion in all sectors of mobility. It should have increased since the last appointment. By this point, you will usually be able to raise your shoulder between 90–120°. The scars should be soft and you can finally sleep on this side. He will prescribe you further physiotherapy to strengthen the muscles and continue improving your passive range of motion. You will also be shown some exercises that you can do at home every day to stretch the joint.
6-MONTH CHECK-UP :
By now the shoulder should be supple and pain-free. The shoulder may not have regained full strength, which can be very hard to achieve. The surgery does not restore the muscles but allows you to use your shoulder in day-to-day life without having to think about it. Patients experience greatly varying outcomes in terms of strength. It all depends on the condition of the muscle before the surgery. This is why it is important not to delay the treatment.