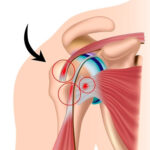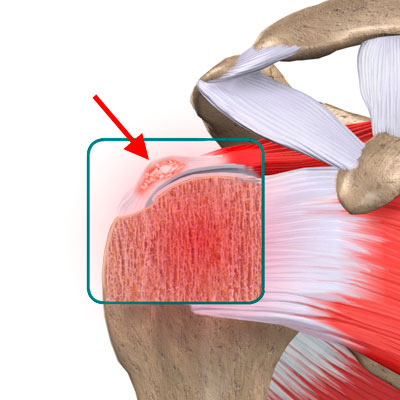
Calcific tendinitis of the rotator cuff tendons (calcification of the shoulder) is a common and very painful shoulder problem that affects mainly young women between the ages of 25 and 50. It may affect just one shoulder or both. The pain is caused by deposits of calcium inside one of more of the rotator cuff tendons. The tendon most commonly affected is the supraspinatus. The pain is severe and happens mainly at night. It can also affect everyday life as it makes it difficult to raise the arms.
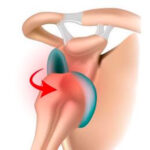
The deposits may stay the same size or they may grow, piercing the tendon and getting resorbed into the subacromial space (between the tendon and the acromion). This resorption is actually part of the natural healing process, although the calcium in the subacromial space triggers an extremely painful inflammatory reaction that lasts 48–72 hours. The pain is so acute that it may require morphine and force patients to seek emergency treatment.

The time to spontaneous resorption varies from a few days to several years, but there is no way of predicting how long it will take. If the pain becomes too crippling, medical treatment maybe offered:
- Steroid injections into the subacromial space, combined with physiotherapy.
- X-ray-guided aspiration, lavage and injections. This is done by a radiologist who inserts a needle into the deposits, guided by x-ray images. As much calcium as possible is then aspirated from the space. This is followed by an injection of steroids to reduce any inflammatory reaction after the procedure.

Neither of these two procedures is 100% effective, especially when the calcification is extensive.
If necessary, Dr Lévy may offer to remove the remaining deposits arthroscopically.
If the deposits are too large, he may also suggest open surgery.

You should keep your arm in a sling night and day for 2–3 weeks after the surgery. If you are very careful or when taking a shower, you can remove your arm from the sling and hold it against your body. You should not raise the arm or actively move it away from the body. Within a few days you can begin a few exercises by yourself that involve gently swinging the arm in a pendulum movement. Dr Lévy will explain how to do these exercises properly. He will also prescribe you some sessions of strictly passive physiotherapy, from day 10 after the surgery. The sutures are resorbable and should fall out within 15–20 days. You should then massage the scars to prevent any subcutaneous adhesions from forming.
POSTOPERATIVE CHECK-UPS :
30-DAY CHECK-UP :
By the time you attend this first check-up, the majority of patients say that the spontaneous night-time pain has disappeared. You should still avoid sleeping on the shoulder, but sleep on your back or on your other side. This appointment is the last time you will need to wear the sling. Dr Lévy will make sure the wounds are healing well and check your passive movement. You will have an x-ray to check the calcium deposits have gone and that the tip of the acromion was cleanly removed. At this point the surgeon will decide whether you can begin active assisted physiotherapy, and increase your passive then active range of motion, depending on the pain. You must continue to massage the scars to prevent any subcutaneous adhesions from forming.
4-MONTH CHECK-UP :
At this appointment, Dr Lévy will check the range of motion in all sectors of mobility. It should have increased since the last appointment. By now, the shoulder will usually have recovered its normal range of motion. The scars should be soft and you can finally sleep on this side. He will prescribe you further physiotherapy to strengthen the muscles and continue improving your passive range of motion. You will also be shown some exercises that you can do at home every day to stretch the joint.
6-MONTH CHECK-UP :
By now the shoulder should be supple and pain-free. You can resume any sports, but should not force the shoulder in case of any residual pain.