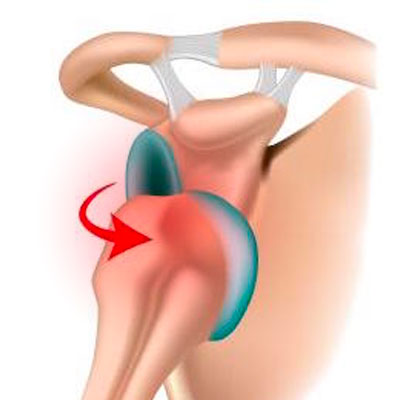
Shoulder instability is a common complaint in young sporting patients and may have many clinical presentations, such as dislocation, subluxation or simply pain when tensing the arm. The shoulder may dislocate forwards (anterior dislocation, 95% of cases) or backwards (posterior dislocation, 5% of cases).

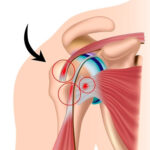
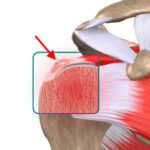
The shoulder is the most mobile joint in the human body but is also the most unstable. It articulates the head of the humerus against the glenoid rim of the shoulder blade. Stability is provided by the glenoid labrum (a fibrous ring of tissue) and the glenohumeral ligaments. When the shoulder dislocates, the glenoid labrum comes away from the glenoid and is no longer able to stabilise the joint. Moreover, every time the joint fully or partially dislocates, the bone on the head of the humerus and shoulder blade gets eroded. The two bones lose contact and the joint become more and more unstable. This is what causes the dislocation to happen again and again. It is known as recurrent dislocation.

The symptoms vary between patients. The shoulder may fully dislocate, possibly requiring another person to put it back in place (dislocation), or it may partially dislocate and go back into place by itself after a few seconds (subluxation); in both cases the diagnosis of shoulder instability is obvious. However, patients may simply experience shoulder pain or apprehension when assuming certain positions, especially before throwing an object or tensing the arm (e.g. when serving in a tennis match). This is known as a painful unstable shoulder.
The condition is often caused by trauma, such as a fall or inadvertent movement. Upon examination, the arm is fully mobile and there is no loss of strength. Tensing the arm may cause pain or apprehension. In particularly young patients, there may be hyperlaxity indicating a minor congenital abnormality in the ligaments which are too loose and make the shoulder more likely to become unstable.
If left untreated, an unstable shoulder will become more and more painful; the problems will occur more often and for smaller and smaller movements. In particular, the joint cartilage will wear away much faster than normal and risk progressing to early-onset osteoarthritis.
 The condition is usually easy to diagnose based on the obvious clinical presentation as the patient describes their dislocations. An x-ray of the dislocated shoulder and a good physical examination are enough to establish a diagnosis.
The condition is usually easy to diagnose based on the obvious clinical presentation as the patient describes their dislocations. An x-ray of the dislocated shoulder and a good physical examination are enough to establish a diagnosis.
However, a particularly thorough physical examination is required for subluxations or painful unstable shoulders. The surgeon should examine both shoulders when the patient is relaxed. X-rays will be taken of both shoulders plus a joint scan of the affected shoulder in order to check for damage to the anterior labrum or any damage to the head of the humerus or glenoid rim. An MRI does not provide much useful information for this condition and is therefore not used.
There are two scenarios for anterior instability :
Recurrent dislocation or subluxation :
A patient who has had two or more episodes of shoulder dislocation or subluxation should be offered surgery to prevent recurrence and developing osteoarthritis
First dislocation in a young sporting subject :
For several years, scientific research has shown that after a young sporting subject (< 25 years) has experienced a first objective shoulder dislocation, the risk of recurrence is greater than 85%. Arthroscopic treatment within four weeks of the incident to reinsert the glenoid labrum reduces this risk to 15%. This is specific to the first episode of true dislocation in an athlete aged under 25 years.
Unstable painful shoulder :
With an unstable painful shoulder, the patient complains only of pain with no feeling of the joint being dislocated. When questioned and with a thorough physical examination as well as further diagnostic tests, the surgeon may find that the pain is actually due to shoulder instability, despite the patient not being aware of it. This then requires a joint scan to determine the damage to the glenoid labrum and bone. This presentation should be treated the same as multiple subluxations. It can also cause cartilage damage and should therefore be treated the same way as an unstable shoulder.

n all three scenarios, the surgeon should consider surgery and decide between two possible treatments. An arthroscopic repair (Bankart) or open surgery (Latarjet bone block) – see the section on Hospital Stay & Procedure.
Posterior instability should be initially treated with physiotherapy which, unlike for anterior instability, can be sufficient to recentre the shoulder and prevent recurrence. If this fails, surgery is the next step (arthroscopy or open surgery, depending on the case).
Arthroscopic repair (Bankart) :
This procedure is performed arthroscopically, which means the surgeon does the operation by inserting a small camera into the joint. The aim is to reattach the glenoid labrum to the glenoid rim using very tiny anchors. The surgeon makes two tiny 5mm incisions which will be invisible within a few months after the surgery.

Open surgery (Latarjet bone block) :
With this operation, a bone block is fixed to the front of the glenoid using a fragment of bone harvested from the shoulder joint and attached to the glenoid using two screws. This bone graft increases the joint surface area and stops the shoulder from dislocating forwards. It leaves a 4cm scar along the deltopectoral groove.

 You should keep your arm in a sling night and day for one month after the surgery. If you are very careful or when taking a shower, you can remove your arm from the sling and hold it against your body. You should not raise the arm or actively move it away from the body. Depending on the procedure, Dr Lévy may prescribe you some physiotherapy involving strictly passive movement which can begin 15 days after a bone block procedure. After an arthroscopic repair (Bankart), physiotherapy can start after the one-month check-up.
You should keep your arm in a sling night and day for one month after the surgery. If you are very careful or when taking a shower, you can remove your arm from the sling and hold it against your body. You should not raise the arm or actively move it away from the body. Depending on the procedure, Dr Lévy may prescribe you some physiotherapy involving strictly passive movement which can begin 15 days after a bone block procedure. After an arthroscopic repair (Bankart), physiotherapy can start after the one-month check-up.
POSTOPERATIVE CHECK-UPS :
30-DAY CHECK-UP :
By this first check-up, the majority of patients say that the spontaneous pain has disappeared. You should still avoid sleeping on the shoulder but sleep on your back or on your other side. This appointment is the last time you will need to wear the sling. Dr Lévy will make sure the wounds are healing well and check your passive movement. An x-ray will be used to check that the screws or implants used to suture the labrum are still in place. At this point the surgeon will decide whether you can begin active assisted physiotherapy, and increase your passive then active range of motion, depending on the pain. You must continue to massage the scars to prevent any subcutaneous adhesions from forming.
3-MONTH CHECK-UP :
At this appointment, Dr Lévy will check the range of motion in all sectors of mobility. It should have increased since the last appointment. By this point, you will usually be able to raise your shoulder between 90–120°. The scars should be soft and you can finally sleep on this side. The surgeon will prescribe you further physiotherapy to strengthen the muscles and continue improving your passive range of motion. You will also be shown some exercises that you can do at home every day to stretch the joint. After a bone block procedure, you will also be referred for an x-ray and bone scan to check the consolidation of the bone graft.
4–5 MONTH CHECK-UP :
By now the shoulder should be supple and pain-free. The shoulder will not yet have regained full strength, which will gradually return over time. You will no longer feel any instability and can resume light sports but should not begin any intense training until the surgeon gives you the go-ahead.